Which nerve innervates the diaphragm? Diaphragm: structure and functions. Functions of the diaphragm in normal physiology
Diaphragm- tendon-muscular formation separating the thoracic and abdominal cavities (Fig. 81). The muscular part of the diaphragm begins along the circumference of the lower aperture of the chest from the sternum, the inner surface of the cartilages of the VII-XII ribs and the lumbar vertebrae (sternal, costal and lumbar sections of the diaphragm).
The muscle bundles go upward and radially and end at the tendon center, forming dome-shaped protuberances on the right and left. Between the sternum and costal region there is a sternocostal space (triangle of Morgagni, Larrey), filled with fiber. The lumbar and costal regions are separated by the lumbocostal space (Bochdalek's triangle). The lumbar diaphragm consists of three legs on each side: external (lateral), intermediate and internal (medial). The tendinous edges of both internal (medial) legs of the diaphragm form an arch at the level of the first lumbar vertebra to the left of the midline, limiting the opening for the aorta and thoracic lymphatic duct. The esophageal opening of the diaphragm is formed in most cases due to the right internal (medial) leg of the diaphragm; the left leg is involved in its formation only in 10% of cases. The vagus nerves also pass through the esophageal opening of the diaphragm. Sympathetic trunks, celiac nerves, azygos and semi-gypsy veins pass through the intermuscular gaps of the lumbar diaphragm. The opening for the inferior vena cava is located in the tendinous center of the diaphragm.

Rice. 81. Topographic anatomy of the diaphragm. Localization of congenital and acquired hernias. 1 - tendon center; 2, 3 - sternocostal space (Larrey, Morgagni triangle); 4 - localization of congenital holes and acquired defects of the diaphragm; 5, 6 - lumbocostal triangles; 7 - esophageal opening of the diaphragm; 8 - aorta; 9 - inferior vena cava.
The diaphragm is covered above by the intrathoracic fascia, pleura and pericardium, and below by the intra-abdominal fascia and peritoneum. Adjacent to the retroperitoneal part of the diaphragm are the pancreas, duodenum, kidneys and adrenal glands, surrounded by a fatty capsule. The liver is adjacent to the right dome of the diaphragm, the spleen, the fundus of the stomach, and the left lobe of the liver are adjacent to the left. There are corresponding ligaments between these organs and the diaphragm. The right dome of the diaphragm is located higher (fourth intercostal space) than the left (fifth intercostal space). The height of the diaphragm depends on the constitution, age, and the presence of various pathological processes in the chest and abdominal cavities.
Blood supply to the diaphragm are carried out by the upper and lower phrenic arteries, which arise from the aorta, the musculo-phrenic and pericardial-phrenic arteries, which arise from the internal thoracic artery, as well as six lower intercostal arteries.
The outflow of venous blood occurs through the veins of the same name, through the azygos and semi-gypsy veins, as well as through the veins of the esophagus.
Lymphatic vessels of the diaphragm form several networks: subpleural, pleural, intrapleural, subperitoneal, peritoneal. Through the lymphatic vessels located along the esophagus, aorta, inferior vena cava and other vessels and nerves passing through the diaphragm, the inflammatory process can spread from the abdominal cavity to the pleural cavity and vice versa. Lymphatic vessels drain lymph from above through the prelaterotropericardial and posterior mediastinal nodes, from below - through the para-aortic and peri-esophageal nodes. The diaphragm is innervated by the phrenic and intercostal nerves.
There are static and dynamic functions of the diaphragm. The statistical function of the diaphragm is to maintain the difference in pressure in the thoracic and abdominal cavities and the normal relationship between their organs. It depends on the tone of the diaphragm. The dynamic function of the diaphragm is due to the effect of the diaphragm moving during breathing on the lungs, heart and abdominal organs. The movements of the diaphragm ventilate the lungs, facilitate the flow of venous blood into the right atrium, promote the outflow of venous blood from the liver, spleen and abdominal organs, the movement of gases in the gastrointestinal tract, the act of defecation, and lymph circulation.
Surgical diseases. Kuzin M.I., Shkrob O.S. et al., 1986
The thoracic obstruction or diaphragm separates the chest cavity from the abdominal cavity. It is divided into two parts: the muscular part, pars muscularis diaphragmaticus, and the tendon center, centrum tendineum.
The tendinous center of the diaphragm, consists of an anterior leaf, folium anterius, and lateral leaves, folium dexter and folium sinister, located in the horizontal plane, and the muscular part is in the vertical plane. The heart is located on the front leaf of the tendon center, and the lungs are on the lateral leaves.
Depending on the attachment sites, the muscular part of the diaphragm is in turn divided into the sternal part of the diaphragm, pars sternalis, the costal part, pars costalis, and the lumbar part, pars lumbalis.
The pedicles of the lumbar part of the diaphragm are as follows:
1. Crus mediale - the medial leg starts from lig. longitudinale anterius and the bodies of the III or IV lumbar vertebrae on the right; on the left one vertebra higher. At the level of the first lumbar vertebra, both legs converge, limiting the aortic opening for the aorta and thoracic duct.
2. Crus intermedius - intermediate leg - starts from the lateral surface of the body of the II lumbar vertebra and above passes into the muscular part of the diaphragm.
Z. Crus laterale - lateral leg - starts from the lateral surface of the body of the II lumbar vertebra with the formation of two tendon arches, representing a thickening of the fascia endoabdominalis.
Arcus lumbocostalis medialis - medial lumbocostal arch - starts from the body of the II lumbar vertebra, spreads over m. psoas major and attaches to the transverse process of the first lumbar vertebra.
Arcus lumbocostalis lateralis - lateral lumbocostal arch - starts from the transverse process of the first lumbar vertebra, spreads over m. quadratus lumborum and is attached to the XII rib.
Trigonum lumbo-costale - the lumbocostal triangle is located between the lumbar and costal parts of the diaphragm. Its base is the lower edge of the XII rib. The bottom of the triangle is lined on the side of the thoracic cavity with pleura, fused with thin fascial sheets, to which the posterior surface of the kidney and adrenal gland, surrounded by a fatty capsule, is adjacent.
Trigonum sterno-costale - the sternocostal triangle lies between the sternum and costal parts of the diaphragm. Its height is from 1.8 to 2.7 cm, its base is from 2.5 to 3 cm.
The diaphragm has the following large holes:
1. Hiatus aorticus - aortic opening - is enclosed between the medial diaphragmatic legs and their tendon part. The aorta and thoracic duct pass through this opening at the level of the XII thoracic vertebra.
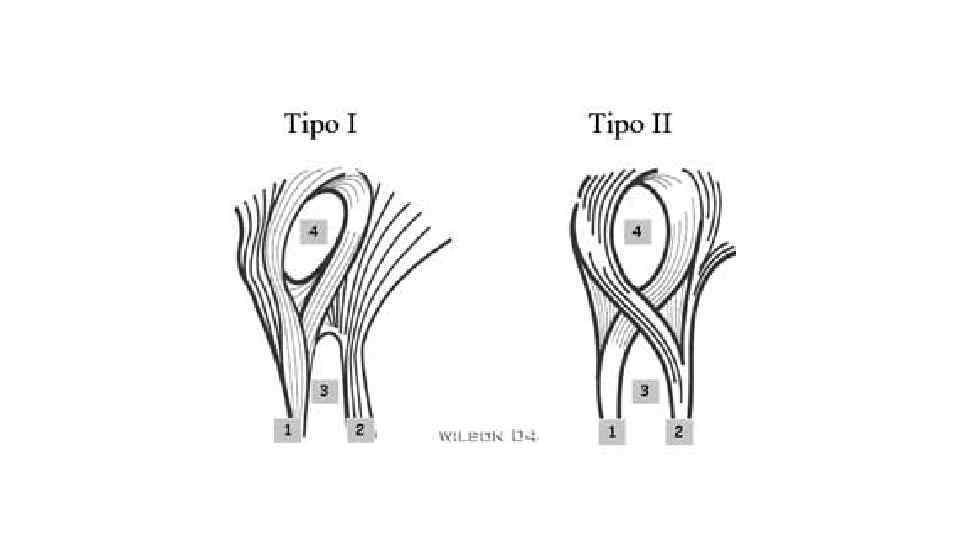
2. Hiatus oesophageus – esophageal opening; The medial diaphragmatic legs, after the formation of the aortic opening, cross and, diverging again, form a second opening in the muscular part, hiatus oesophageus, through which the esophagus and vagus nerves pass. In the lumbar part of the diaphragm there are two openings formed in the shape of a figure eight: the lower one is the aortic (tendon) and the upper one is the esophageal (muscular).
Z. Foramen quadrilaterum s. venae cavae inferioris - the four-sided opening of the inferior vena cava - is located in the right sheet of the tendon center of the diaphragm, through which the inferior vena cava passes.
Blood supply to the diaphragm. The anterolateral parts of the periphery of the diaphragm are supplied with blood due to aa. intercostales and its anterior section from aa. pericardiacophrenicae and aa. intercostales. Thus, the system of branches of the descending aorta, thoracic and abdominal sections, and the subclavian arteries takes part in the circuitous circulation of the diaphragm.
A. phrenica superior supplies blood to the lumbar part of the diaphragm from the side of the thoracic cavity and the pleura covering it. A. phrenica inferior supplies blood to the diaphragm and peritoneum; the left, in addition, the final part of the esophagus, and the right - the wall of the inferior vena cava, the inferior phrenic veins, vv. phrenicae inferioris, adjacent in two to the artery of the same name, flows into the inferior vena cava.
Innervation of the diaphragm. N. phrenicus - the phrenic nerve arises from the anterior branches of the III-IV cervical nerves. The left phrenic nerve penetrates the diaphragm and branches on its lower surface; the right one ends with its branches on the upper surface of the diaphragm. 6 lower intercostal nerves take part in the innervation of the posterior part of the diaphragm.
Funnel chest deformity- a congenital defect associated with hyperplasia of the cartilage and the lower pairs of ribs themselves. The body of the sternum is displaced posteriorly, forming a depression. The deformity is often asymmetrical, and the severity of the defect varies greatly. Keeled chest shape - protruding deformity of the sternum, less common than funnel-shaped deformity.
Amastia- a pathology of fetal development, as a result of which a person is born without one or both mammary glands. With amastia, breastfeeding becomes impossible and may be accompanied by defects in the ovaries or other body systems, which leads to disruption of the development of the entire reproductive system. Such a woman has neither breast tissue nor a nipple. Polymastia- the presence of accessory, multiple glands and nipples, representing developed glands or underdeveloped ones, with clear nipples, located along the “milk line”, which runs from the armpits to the inguinal-femoral region. It is more common in women, and during lactation the accessory glands can swell and secrete milk.
Gynecomastia– enlargement of the mammary gland in men with hypertrophy of glands and adipose tissue. Painful asymmetrical thickening of the mammary glands often occurs, which disappears spontaneously. The size of the magnification may vary. Physiological gynecomastia occurs in newborns, during puberty and in older men. There is a pathological form of gynecomastia.
Diaphragmatic hernia- protrusion of the esophagus, stomach or small intestine through the diaphragm into the chest cavity. This disrupts the functioning of the esophageal sphincter, which closes the transition from the esophagus to the stomach.
Aplasia of the diaphragm– anomalies in the development of the diaphragm, in which part of the diaphragm or a fragment of any part is missing. In newborns, there is a congenital absence of the entire diaphragm, which is incompatible with life. There are unilateral and total aplasia of the diaphragm. Unilateral aplasia can be complete or partial.
Relaxation of the diaphragm– relaxation of the domes and high standing of the diaphragm, which is based on paralysis, sharp thinning and persistent displacement of it into the chest along with the adjacent abdominal organs. Congenital relaxation of the diaphragm is associated with aplasia or underdevelopment of its muscular part, as well as intrauterine injury or aplasia of the phrenic nerve. Acquired relaxation occurs due to secondary atrophy, damage to the phrenic nerve, or damage to the diaphragm itself by injury or tumor.
The lower wall of the chest cavity is represented by a muscular septum - the diaphragm, which with its dome rises upward - on the right to the level of the cartilage of the IV rib and on the left to the level of the V rib. During acts of breathing, the diaphragm moves by 2-3 cm.
The diaphragm consists of a tendon center - centrum tendineum and muscle bundles converging to it (Fig. 115).
Rice. 115. Diaphragm.
1 - trigonum sternocostale sinister (Larrey's fissure); 2 - sternum; 3 - pars sternalis diaphragmatis and trigonum sternocostale dexter (Morgagni gap); 4 - diaphragmatic part of the pericardium; 5 - v. cava inferior; 6 - n. phrenicus; 7 - parscostalis diaphragmatis; 8 - nn. vagi; 9 - esophagus; 10 - v. azygos; 11 - thoracic lymphatic duct; 12 - trigonum lumbocostale (Bochdalek gap); 13 - pars lumbalis diaphragmatis; 14 - truncus sympathicus; 15 - thoracic aorta; 16 - tendon center of the diaphragm. Legs of the diaphragm: I - internal; II - average; III - external; 17 - m. quadratus lumborum; 18 - m. psoas; 19 - azygos and n. splanchnicus; 20 - truncus sympathicus.
According to the fixation test, these muscles are divided into parts: the sternal (pars sternalis), starting from the xiphoid process, the costal (pars costalis), starting from the VII-XII ribs, and the lumbar (pars lumbalis) - from the lumbar spine. The right and left halves of the lumbar part of the diaphragm are formed into legs: 1) internal (crus mediale), starting from the bodies of the XII thoracic and the first 3-4 lumbar vertebrae, 2) middle, or intermediate (crus intermedius), following from the body of the II-III lumbar vertebra, and 3) external (crus laterale), extending upward from the internal and external Hallerian arches. The internal arches (arcus lumbocostalis medialis) are stretched from the body of the I or II lumbar vertebra to its transverse process. The external arches (arcus lumbocostalis lateralis) follow from the transverse process of the mentioned vertebra to the free edge of the XII rib. From under the first arch comes the psoas major muscle (m. psoas major), from under the second - the quadratus lumborum muscle (m. quadratus lumborum).
The diaphragm has a series of holes. The inner legs of its lumbar part, fixed to the spine, form a cross in the form of a figure 8, thereby limiting the two holes. The esophagus and the accompanying vagus nerves pass through the anterior opening (hiatus oesophageus), through the posterior opening (hiatus aorticus) the aorta with the surrounding nerve plexus, and behind it the lymphatic duct. The gap between the internal and middle legs contains the azygos (right) and semi-unpaired (left) veins, the greater and lesser splanchnic nerves (the latter can pierce the middle leg). Between the middle and outer legs is the border trunk of the sympathetic nervous system. The tendon part of the diaphragm has an opening for the inferior vena cava (for. venae cavae inferior). The diaphragm still has small, triangular-shaped spaces free from muscle: 1) between the sternum and costal part - trigonum sternocostale of Morgagni (right) and Larrey (left), allowing a. et v. epigastrica superiores, and 2) between the lumbar and costal parts - Bochdalek's trigonum lumbocostale. Through holes in the diaphragm, a hernia may form and the infiltrate may spread.
The diaphragm is supplied with blood from the aa approaching above from the aorta. phrenicae superiores) branches from the internal thoracic artery: aa. musculophrenica, pericardiacophrenica and following below from the aorta aa. phrenicae inferiores and branches from aa. intercostales. Venous blood flows through the aa. pericardia-cophrenicae et vv. phrenicae into the hollow and intercostal veins. The main lymphatic pathways drain lymph to the mediastinal nodes. Innervation is carried out by the phrenic and VII-XII intercostal nerves.
Inside the chest cavity there are two pleural sacs surrounding the lungs, and the mediastinum is the space between these sacs.
 ...The diaphragm... says: “Thanks to me you live, because of me you will die. I hold in my hands the power of life and death; learn to understand me and then you will be calm.” A. T. Still
...The diaphragm... says: “Thanks to me you live, because of me you will die. I hold in my hands the power of life and death; learn to understand me and then you will be calm.” A. T. Still
 The diaphragm is a movable tendon-muscular partition between the thoracic and abdominal cavities. It has a dome shape due to its position internal organs and the difference in pressure in the chest and abdominal cavities. The convex side is directed into the chest cavity, the concave side is directed down into the abdominal cavity. The diaphragm is the main respiratory muscle and the most important abdominal organ
The diaphragm is a movable tendon-muscular partition between the thoracic and abdominal cavities. It has a dome shape due to its position internal organs and the difference in pressure in the chest and abdominal cavities. The convex side is directed into the chest cavity, the concave side is directed down into the abdominal cavity. The diaphragm is the main respiratory muscle and the most important abdominal organ
 In the diaphragm, a muscle part and a tendon center are distinguished. The muscle bundles come from the periphery and have a muscle or tendon origin. Converging upward from the periphery to the middle of the diaphragm, the muscle bundles pass into the tendon center.
In the diaphragm, a muscle part and a tendon center are distinguished. The muscle bundles come from the periphery and have a muscle or tendon origin. Converging upward from the periphery to the middle of the diaphragm, the muscle bundles pass into the tendon center.
 Lumbar part Costal part Sternal part C According to the places where the muscle bundles begin, they are distinguished:
Lumbar part Costal part Sternal part C According to the places where the muscle bundles begin, they are distinguished:
 Lumbar part starts from the anterior surface of the lumbar vertebrae with three pairs of legs: Medial legs Intermediate legs Lateral legs
Lumbar part starts from the anterior surface of the lumbar vertebrae with three pairs of legs: Medial legs Intermediate legs Lateral legs
 Medial legs The right medial leg is more developed and starts from the bodies L 1 -L 4, and the left leg originates from L 1 -L 3. Below, both legs are woven into the anterior longitudinal ligament of the spine, and at the top their fibers cross in front of the body L 1, limiting aortic opening. The aorta and thoracic lymphatic duct pass through this opening.
Medial legs The right medial leg is more developed and starts from the bodies L 1 -L 4, and the left leg originates from L 1 -L 3. Below, both legs are woven into the anterior longitudinal ligament of the spine, and at the top their fibers cross in front of the body L 1, limiting aortic opening. The aorta and thoracic lymphatic duct pass through this opening.
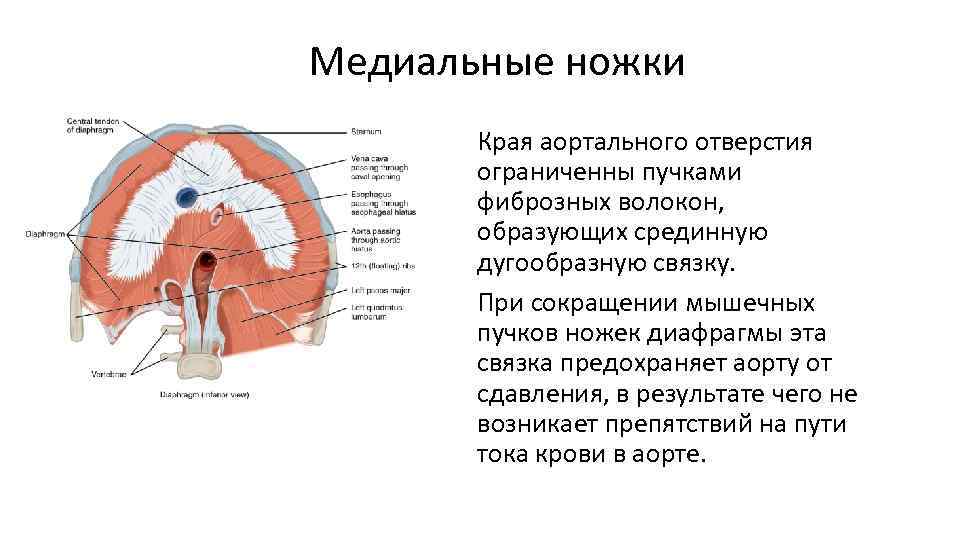 Medial legs The edges of the aortic opening are bounded by bundles of fibrous fibers that form the median arcuate ligament. When the muscle bundles of the legs of the diaphragm contract, this ligament protects the aorta from compression, as a result of which there are no obstacles to the blood flow in the aorta.
Medial legs The edges of the aortic opening are bounded by bundles of fibrous fibers that form the median arcuate ligament. When the muscle bundles of the legs of the diaphragm contract, this ligament protects the aorta from compression, as a result of which there are no obstacles to the blood flow in the aorta.
 Esophageal opening of the diaphragm The esophagus and vagus nerves pass through. The ligament (muscle) of Treitz extends from this area to the duodenojejunal junction.
Esophageal opening of the diaphragm The esophagus and vagus nerves pass through. The ligament (muscle) of Treitz extends from this area to the duodenojejunal junction.

 The intermediate legs are the weakest. They begin lateral to the medial legs of the diaphragm from the lateral surface of L 2 and also go to the center.
The intermediate legs are the weakest. They begin lateral to the medial legs of the diaphragm from the lateral surface of L 2 and also go to the center.
 Lateral crura Originate from the medial and lateral arcuate ligaments and also go to the center
Lateral crura Originate from the medial and lateral arcuate ligaments and also go to the center
 Medial arcuate ligament Stretched over the psoas major muscle between the body of L 1 and the apex of its transverse process
Medial arcuate ligament Stretched over the psoas major muscle between the body of L 1 and the apex of its transverse process
 The psoas muscle passes under the medial arcuate ligament of the PPM Association: - kidneys - C 0 -C 1 - Th 11 -12 - emotions: fear of death; sexual indecisiveness - kidney meridian
The psoas muscle passes under the medial arcuate ligament of the PPM Association: - kidneys - C 0 -C 1 - Th 11 -12 - emotions: fear of death; sexual indecisiveness - kidney meridian
 Lateral arcuate ligament Covers the quadratus lumborum muscle in front, spreading over it from the top of the transverse process of L 1 to the 12th rib. Between the legs of the lumbar part of the diaphragm there are two paired slits. The sympathetic trunk passes into the gap between the intermediate and lateral crura.
Lateral arcuate ligament Covers the quadratus lumborum muscle in front, spreading over it from the top of the transverse process of L 1 to the 12th rib. Between the legs of the lumbar part of the diaphragm there are two paired slits. The sympathetic trunk passes into the gap between the intermediate and lateral crura.
 Quadratus lumborum Associations: - colon - ileocecal valve - L 2 - emotions: guilt; unworthiness of love - colon meridian
Quadratus lumborum Associations: - colon - ileocecal valve - L 2 - emotions: guilt; unworthiness of love - colon meridian
 On each side of the diaphragm, between the lumbar and costal parts of the diaphragm, there is a triangular-shaped area devoid of muscle fibers - the lumbocostal triangle. Here, the abdominal cavity is separated from the thoracic cavity only by thin plates of intra-abdominal and intrathoracic fascia and the serous membranes of the peritoneum and pleura. The same triangular areas exist between the sternum and the costal parts of the diaphragm - the sternocostal triangle. Diaphragmatic hernias can form within these triangles.
On each side of the diaphragm, between the lumbar and costal parts of the diaphragm, there is a triangular-shaped area devoid of muscle fibers - the lumbocostal triangle. Here, the abdominal cavity is separated from the thoracic cavity only by thin plates of intra-abdominal and intrathoracic fascia and the serous membranes of the peritoneum and pleura. The same triangular areas exist between the sternum and the costal parts of the diaphragm - the sternocostal triangle. Diaphragmatic hernias can form within these triangles.
 Costal part of the diaphragm Starts from the inner surface of the 6-7 lower ribs with separate muscle bundles that are wedged between the teeth of the transverse abdominal muscle. The diaphragm muscle bundles are directed upward and inward and pass into the tendon center.
Costal part of the diaphragm Starts from the inner surface of the 6-7 lower ribs with separate muscle bundles that are wedged between the teeth of the transverse abdominal muscle. The diaphragm muscle bundles are directed upward and inward and pass into the tendon center.
 The sternal part of the diaphragm is the narrowest and weakest, starting from the posterior surface of the sternum in the area of the xiphoid process.
The sternal part of the diaphragm is the narrowest and weakest, starting from the posterior surface of the sternum in the area of the xiphoid process.
 Tendon center Muscle bundles of all parts of the diaphragm, moving towards the center, pass into tendon centers, forming a tendon center that looks like a trefoil. On the front petal of this trefoil lies the heart, and in the right petal there is a quadrangular hole through which the inferior vena cava passes.
Tendon center Muscle bundles of all parts of the diaphragm, moving towards the center, pass into tendon centers, forming a tendon center that looks like a trefoil. On the front petal of this trefoil lies the heart, and in the right petal there is a quadrangular hole through which the inferior vena cava passes.
 The entire diaphragm in a relaxed state has the shape of a beveled spherical convexity facing the chest. It has two domes - right and left. The apex of the domes reaches along the parasternal line on the right the level of the 4th intercostal space, and on the left - the 5th intercostal space.
The entire diaphragm in a relaxed state has the shape of a beveled spherical convexity facing the chest. It has two domes - right and left. The apex of the domes reaches along the parasternal line on the right the level of the 4th intercostal space, and on the left - the 5th intercostal space.
 The level of the diaphragm dome is Right Left in the middle. IV rib of the clavicular line along the anterior V rib of the axillary line V rib along the middle VI rib of the axillary line VII rib along the posterior VII rib of the axillary line VIII rib VI rib along the scapular line Seventh intercostal space Eighth intercostal space or VIII rib or IX rib along the paravertebral Eighth intercostal space Ninth intercostal line or IX rib or X rib
The level of the diaphragm dome is Right Left in the middle. IV rib of the clavicular line along the anterior V rib of the axillary line V rib along the middle VI rib of the axillary line VII rib along the posterior VII rib of the axillary line VIII rib VI rib along the scapular line Seventh intercostal space Eighth intercostal space or VIII rib or IX rib along the paravertebral Eighth intercostal space Ninth intercostal line or IX rib or X rib
 Openings of the diaphragm Aortic opening - aorta and thoracic lymphatic duct Esophageal opening - esophagus and vagus nerve Internal arcuate ligament - psoas muscle External arcuate ligament - quadratus lumborum muscle Between the internal and intermediate legs - celiac nerves, v. azigos on the right and v. hemiazigos on the left. Between the lateral and intermediate crura: sympathetic trunk; opening of the inferior vena cava - in the tendon center; sternocostal triangle: superior epigastric artery and veins
Openings of the diaphragm Aortic opening - aorta and thoracic lymphatic duct Esophageal opening - esophagus and vagus nerve Internal arcuate ligament - psoas muscle External arcuate ligament - quadratus lumborum muscle Between the internal and intermediate legs - celiac nerves, v. azigos on the right and v. hemiazigos on the left. Between the lateral and intermediate crura: sympathetic trunk; opening of the inferior vena cava - in the tendon center; sternocostal triangle: superior epigastric artery and veins

 Innervation of the diaphragm Motor nerve phrenic nerve (n. frenicus) Comes out from C 3 -C 5 (cervical plexus)
Innervation of the diaphragm Motor nerve phrenic nerve (n. frenicus) Comes out from C 3 -C 5 (cervical plexus)

 Innervation of the diaphragm The phrenic nerve is also a sensory nerve. It innervates the entire posterior surface of the peritoneum, covering the diaphragm, part of the liver and the posterior part of the spleen and pancreas, adrenal glands, and gall bladder. It forms anastomoses in the solar plexus.
Innervation of the diaphragm The phrenic nerve is also a sensory nerve. It innervates the entire posterior surface of the peritoneum, covering the diaphragm, part of the liver and the posterior part of the spleen and pancreas, adrenal glands, and gall bladder. It forms anastomoses in the solar plexus.

 Innervation of the diaphragm Autonomic innervation Parasympathetic innervation of the diaphragm is provided by the vagus nerves. Sympathetic innervation is provided by the branches of the solar plexus.
Innervation of the diaphragm Autonomic innervation Parasympathetic innervation of the diaphragm is provided by the vagus nerves. Sympathetic innervation is provided by the branches of the solar plexus.
 Innervation of the diaphragm Thus, the fibers of both legs that enter the left side of the tendon center receive their innervation from the left phrenic nerve, and those fibers that enter the tendinous center on the right are supplied from the right phrenic nerve. The lower 6 or 7 intercostal nerves distribute sensory fibers to the peripheral part of the muscles, the sensory sensitivity of these nerves is confirmed by absolute muscle atrophy on the side of the destruction of the phrenic nerve.
Innervation of the diaphragm Thus, the fibers of both legs that enter the left side of the tendon center receive their innervation from the left phrenic nerve, and those fibers that enter the tendinous center on the right are supplied from the right phrenic nerve. The lower 6 or 7 intercostal nerves distribute sensory fibers to the peripheral part of the muscles, the sensory sensitivity of these nerves is confirmed by absolute muscle atrophy on the side of the destruction of the phrenic nerve.
 Blood supply to the diaphragm Thoracic aorta Abdominal aorta Pericardial phrenic Upper and lower diaphragmatic Posterior intercostal
Blood supply to the diaphragm Thoracic aorta Abdominal aorta Pericardial phrenic Upper and lower diaphragmatic Posterior intercostal

 Neurolymphatic reflex Chapman reflex Along the entire length of the sternum. When this reflex is active, this area is very painful.
Neurolymphatic reflex Chapman reflex Along the entire length of the sternum. When this reflex is active, this area is very painful.

 Emotional connections Depression, constant emotional stress, impossibility of achieving assigned tasks. With an excessive emotional reaction, a person always activates breathing, creating an increased biomechanical load for the diaphragm, which leads to multidirectional contraction of its muscle fibers.
Emotional connections Depression, constant emotional stress, impossibility of achieving assigned tasks. With an excessive emotional reaction, a person always activates breathing, creating an increased biomechanical load for the diaphragm, which leads to multidirectional contraction of its muscle fibers.
 The development of the diaphragm is laid at the level of C 4 -C 5 from the mesoderm. The chest organs and the phrenic nerve are located nearby. On the sides is the falciform ligament (the future pleuroperitoneal canal). By 8 weeks it moves down, reaching the level of the chest, and all elements fuse together. 8 -9 weeks - connective tissue membrane 23 weeks - muscular organ In case of developmental defects, the pleuroperitoneal canal does not heal or hernias form due to underdevelopment (nonunion) of the components.
The development of the diaphragm is laid at the level of C 4 -C 5 from the mesoderm. The chest organs and the phrenic nerve are located nearby. On the sides is the falciform ligament (the future pleuroperitoneal canal). By 8 weeks it moves down, reaching the level of the chest, and all elements fuse together. 8 -9 weeks - connective tissue membrane 23 weeks - muscular organ In case of developmental defects, the pleuroperitoneal canal does not heal or hernias form due to underdevelopment (nonunion) of the components.


 Physiology of breathing Inhalation 1. Caudal displacement of the diaphragm. Active tension of the muscles located around the circumference of the tendon center. The muscles move away from the fixed base of the lower ribs, lowering the dome of the diaphragm and displacing the abdominal organs caudally. The 12th rib must be well fixed by the quadratus lumborum muscle so that the diaphragm can provide maximum pressure on the abdominal organs.
Physiology of breathing Inhalation 1. Caudal displacement of the diaphragm. Active tension of the muscles located around the circumference of the tendon center. The muscles move away from the fixed base of the lower ribs, lowering the dome of the diaphragm and displacing the abdominal organs caudally. The 12th rib must be well fixed by the quadratus lumborum muscle so that the diaphragm can provide maximum pressure on the abdominal organs.
 Physiology of breathing Inhalation Purpose: active stretching of the lower lobes of the lungs with air. Stabilizing muscles: scalene, sternocleidomastoid create a fixation point from which the diaphragm begins to move (prevent the shoulder girdle from moving downwards).
Physiology of breathing Inhalation Purpose: active stretching of the lower lobes of the lungs with air. Stabilizing muscles: scalene, sternocleidomastoid create a fixation point from which the diaphragm begins to move (prevent the shoulder girdle from moving downwards).
 Physiology of breathing Inhalation 2. Lateral movement - contraction of the external intercostal muscles. Goal: active stretching of the middle lobes of the lungs with air. Stabilizing muscles: quadratus lumborum muscle. At the moment when the movement of the internal organs reaches its limit, the tendon center becomes a point of fixation. The diaphragm first raises the lower ribs, then the upper ones to expand the chest.
Physiology of breathing Inhalation 2. Lateral movement - contraction of the external intercostal muscles. Goal: active stretching of the middle lobes of the lungs with air. Stabilizing muscles: quadratus lumborum muscle. At the moment when the movement of the internal organs reaches its limit, the tendon center becomes a point of fixation. The diaphragm first raises the lower ribs, then the upper ones to expand the chest.
 Physiology of breathing Inhalation 3. Ventral displacement – contraction of the anterior internal intercostal muscles. Goal: active stretching of the upper lobes of the lungs with air. Stabilizing muscles: no. Movement is ensured by the elasticity of the pericardial sternal ligaments.
Physiology of breathing Inhalation 3. Ventral displacement – contraction of the anterior internal intercostal muscles. Goal: active stretching of the upper lobes of the lungs with air. Stabilizing muscles: no. Movement is ensured by the elasticity of the pericardial sternal ligaments.
 Physiology of breathing Exhalation Quiet exhalation is passive (the diaphragm relaxes). The auxiliary muscles of the chest and abdomen are involved in forced exhalation.
Physiology of breathing Exhalation Quiet exhalation is passive (the diaphragm relaxes). The auxiliary muscles of the chest and abdomen are involved in forced exhalation.


 Structures of the nervous system and large vessels associated with the diaphragm Thoracic sympathetic chain. Solar plexus + splanchnic nerve, large and small. Intercostal nerves Th 6 - Th 12. Vagus nerve. Abdominal aorta, celiac trunk. Thoracic lymphatic duct.
Structures of the nervous system and large vessels associated with the diaphragm Thoracic sympathetic chain. Solar plexus + splanchnic nerve, large and small. Intercostal nerves Th 6 - Th 12. Vagus nerve. Abdominal aorta, celiac trunk. Thoracic lymphatic duct.
 Organs associated with the diaphragm Internal organs lying above the diaphragm in the chest. - heart, lungs, esophagus, large vessels. Internal organs lying below the diaphragm in the abdominal cavity. - kidneys, liver, stomach, pancreas, spleen; large intestine, small intestine.
Organs associated with the diaphragm Internal organs lying above the diaphragm in the chest. - heart, lungs, esophagus, large vessels. Internal organs lying below the diaphragm in the abdominal cavity. - kidneys, liver, stomach, pancreas, spleen; large intestine, small intestine.

 Clinical manifestations of diaphragm dysfunction. - pain or feeling of tension in the thoracolumbar junction; - pain under the costal arch; - posture disorders; - respiratory diseases (including bronchitis, bronchial asthma, sinusitis); - diseases of the digestive system (the abdominal organs have a direct or indirect ligamentous connection with the diaphragm)
Clinical manifestations of diaphragm dysfunction. - pain or feeling of tension in the thoracolumbar junction; - pain under the costal arch; - posture disorders; - respiratory diseases (including bronchitis, bronchial asthma, sinusitis); - diseases of the digestive system (the abdominal organs have a direct or indirect ligamentous connection with the diaphragm)
 Clinical manifestations of the diaphragm Disorders of peripheral circulation in the lower extremities associated with pathology of the inferior vena cava and abdominal aorta; Lymphocirculation disorders (including edema of the lower extremities and abdominal edema); Urogenital disorders (the kidneys are in direct connection with the diaphragm). TO
Clinical manifestations of the diaphragm Disorders of peripheral circulation in the lower extremities associated with pathology of the inferior vena cava and abdominal aorta; Lymphocirculation disorders (including edema of the lower extremities and abdominal edema); Urogenital disorders (the kidneys are in direct connection with the diaphragm). TO
 Clinical manifestations of diaphragm dysfunction Instability of L 5 -S 1, which forms a disc herniation Diaphragmatic hernia (heartburn, belching, chest pain) Manifestations of weakness of the quadratus lumborum muscle Manifestations of weakness of the iliopsoas muscle
Clinical manifestations of diaphragm dysfunction Instability of L 5 -S 1, which forms a disc herniation Diaphragmatic hernia (heartburn, belching, chest pain) Manifestations of weakness of the quadratus lumborum muscle Manifestations of weakness of the iliopsoas muscle
 Pathobiomechanics of the diaphragm. According to L.F. Vasilyeva Disturbances of the thoraco-abdominal diaphragm in more than 50% of cases are the cause of human diseases. Respiratory disorders cause: 1. Autonomic imbalance, squeezing the vagus nerve and disrupting the trophism of organs; 2. Formation of the biomechanics of the endorhythm of internal organs, ensuring their ligamentous imbalance; Changes the activity of the craniosacral rhythm because each stage of breathing affects the activity of specific bones of the skull. Reduced energy activity of the front and rear energy meridians, which leads to loss large quantity energy.
Pathobiomechanics of the diaphragm. According to L.F. Vasilyeva Disturbances of the thoraco-abdominal diaphragm in more than 50% of cases are the cause of human diseases. Respiratory disorders cause: 1. Autonomic imbalance, squeezing the vagus nerve and disrupting the trophism of organs; 2. Formation of the biomechanics of the endorhythm of internal organs, ensuring their ligamentous imbalance; Changes the activity of the craniosacral rhythm because each stage of breathing affects the activity of specific bones of the skull. Reduced energy activity of the front and rear energy meridians, which leads to loss large quantity energy.
 An enlargement of the esophageal opening leads to compression of the cardiac part of the stomach, disrupting its main function - the breakdown of complex proteins into simple amino acids, and a person cannot digest protein foods, with all the ensuing consequences, not to mention the fact that the iliopsoas muscle is woven into the legs of the diaphragm and a decrease in its tone leads to nephroptosis. In addition, the diaphragm is influenced by 8 internal organs that are attached to it. But the most common imbalance problem is associated with neck instability, as a result of which the upper cervical spine is blocked and any movement is accompanied by overload of the mid-cervical spine, constantly compressing the phrenic nerve.
An enlargement of the esophageal opening leads to compression of the cardiac part of the stomach, disrupting its main function - the breakdown of complex proteins into simple amino acids, and a person cannot digest protein foods, with all the ensuing consequences, not to mention the fact that the iliopsoas muscle is woven into the legs of the diaphragm and a decrease in its tone leads to nephroptosis. In addition, the diaphragm is influenced by 8 internal organs that are attached to it. But the most common imbalance problem is associated with neck instability, as a result of which the upper cervical spine is blocked and any movement is accompanied by overload of the mid-cervical spine, constantly compressing the phrenic nerve.

 Types of diaphragm dysfunction Inspiratory dysfunction - the inhalation phase is greater than the exhalation phase - 90% Expiratory dysfunction - the expiratory phase is greater than the inhalation phase - 10% Inspiratory dysfunction - 1st degree dysfunction (maintaining the suction action of the diaphragm) 2nd degree dysfunction (without maintaining the suction action) Primary, secondary
Types of diaphragm dysfunction Inspiratory dysfunction - the inhalation phase is greater than the exhalation phase - 90% Expiratory dysfunction - the expiratory phase is greater than the inhalation phase - 10% Inspiratory dysfunction - 1st degree dysfunction (maintaining the suction action of the diaphragm) 2nd degree dysfunction (without maintaining the suction action) Primary, secondary
 Diaphragm testing 4 stages of diagnosis Calm breathing. Forced breathing - diagnosis of domes. Forced breathing - diagnosis of ribs. Diagnosis of the crura of the diaphragm (through the costovertebral triangle).
Diaphragm testing 4 stages of diagnosis Calm breathing. Forced breathing - diagnosis of domes. Forced breathing - diagnosis of ribs. Diagnosis of the crura of the diaphragm (through the costovertebral triangle).
 Vertebral costal triangle Petit or Greenfeld triangle. SPACE: Under the 12th rib, lateral to the quadratus lumborum muscle
Vertebral costal triangle Petit or Greenfeld triangle. SPACE: Under the 12th rib, lateral to the quadratus lumborum muscle
 Correction techniques Techniques for correcting trigger points. Non-specific dome correction techniques - “umbrella” technique, axial twisting, inhibition. Specific techniques for correcting one of the domes - for diaphragm dysfunction of degrees 1 and 2. Correction of the legs of the diaphragm. Correction of the sternum. Final technology - technology triangles. Fascial techniques.
Correction techniques Techniques for correcting trigger points. Non-specific dome correction techniques - “umbrella” technique, axial twisting, inhibition. Specific techniques for correcting one of the domes - for diaphragm dysfunction of degrees 1 and 2. Correction of the legs of the diaphragm. Correction of the sternum. Final technology - technology triangles. Fascial techniques.


